




Swallowing difficulties and dysphagia
Understanding dysphagia and its causes.
What is dysphagia?[1]
Dysphagia is the medical term to describe difficulty in swallowing. This includes problems with:
- Sucking
- Swallowing
- Drinking
- Chewing
- Eating
- Dribbling saliva
- Closing your lips
Eating and drinking is a vital part of life. Difficulty swallowing can limit what you can eat and drink, leading to frustration, stress and health problems.
What are the symptoms of dysphagia? [1]
Signs and symptoms associated with dysphagia include:
- Gagging or choking when eating or drinking
- Food or drink getting stuck in your throat or going down the “wrong way”
- Eating a meal takes a long time (more than 30 minutes)
- The need to cough or clear your throat during or after eating and drinking
- Being short of breath when eating and drinking
- Avoiding some foods because they are hard to swallow
- Regular chest infections for no obvious reason
Babies that have difficulty sucking during breast or bottle feeding can also have dysphagia. [1]
A surprisingly high proportion of adults are unable to swallow tablets or capsules as highlighted in a survey of patients aged over 60 years carried out by community pharmacists; almost 60% of the 792 respondents experienced difficulty in swallowing medication in this form. A similar proportion reported opening capsules or crushing tablets to make ingestion easier, unaware of the negative effect it may have on the activity of the drug.[2]
Doctors are often unaware that their patient has an issue with the formulation of their medicine. It is important, therefore, for prescribers and other healthcare professionals to assess if the patient has swallowing difficulties, which may affect adherence.[2]
Swallowing difficulty, or dysphagia, can occur in any age group although it is most common in older people since they are more prone to the causative diseases and age-related changes in salivary gland function. Up to one-third of residents in nursing homes may experience difficulty swallowing, resulting in the common practice of crushing or opening of medicines. NICE guidance on managing medicines in care homes recommends the identification of swallowing problems as an integral element of the medication review process. [3]
Patients with swallowing difficulties present a management challenge since: [2]
- Therapeutic outcomes may be affected in those not adhering to prescribed medications.
- Tablets or capsules may cause choking with consequent risk to the airway. [2]
- There may be an increased risk of a tablet or capsule becoming lodged in the patient’s throat or oesophagus, resulting in incorrect drug dispersal and subsequent changes in efficacy and/or tolerability, and possible oesophageal damage. [2]
Causes of dysphagia and related swallowing problems
Dysphagia describes any impairment of the swallowing process. Dysphagia is not a disease, but a symptom caused by a structural or neurological dysfunction.[4]
The causes of swallowing difficulties are numerous, manifesting as mechanical obstruction, or affecting the muscles or nerves involved in swallowing.[2]
Consider individual investigation and management in the following conditions: [2]
- neurological conditions (e.g. stroke, progressive neurological disease)
- cancer (e.g. head, neck, oesophageal cancer)
- cardiac and respiratory disease
- physical/learning disabilities
The ‘normal’ swallow needs the respiratory, oral, pharyngeal, laryngeal and oesophageal structures to function with one another. This is dependent on the motor and sensory nervous system being intact.[5]
There are three main phases to the normal swallow which are reliant on both motor activity and sensory feedback: [4]
Figure 1 – Oral Phase [4]
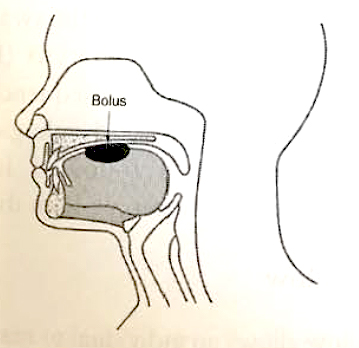
Figure 2 – Pharyngeal Phase [4]
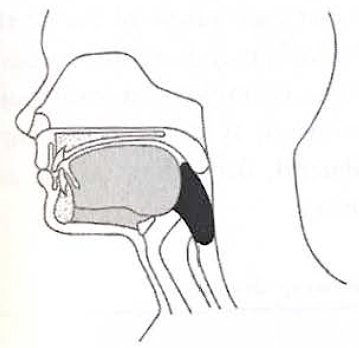
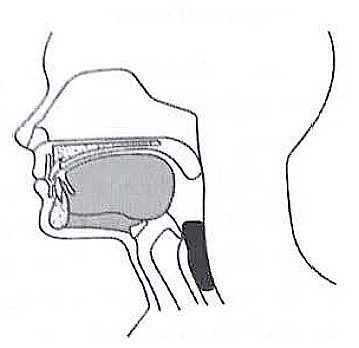
Figure 3 – Oesophageal Phase [4]
Any of these phases can malfunction to produce swallowing problems, i.e. ‘dysphagia’- these are set out in the table below:[4]
Table 1 – Normal Function & Malfunction (adapted from Wright et al. 2011)[4]
| Phase | Normal function | Malfunction |
|---|---|---|
| Oral | Preparation of food and drink for transit into the pharynx. Once the preparation is complete, a bolus is formed. At the end of the phase, the bolus is propelled backward towards the pharynx by the tongue. | Failure to detect material within the mouth can be caused by a sensory or cognitive disturbance. Uncontrolled material may spill from the lips or into the pharynx. Altered muscle tone affects the action of the jaw, lips, tongue and soft palate disrupting the retention and preparation of the bolus. |
| Pharyngeal | Provides a mechanism to prevent material entering the airway. The main activities are the cessation of breathing and closure of the airway. | Aspiration prior to the swallow – Loss of sensation within the pharynx results in absent or delayed initiation of the pharyngeal phase. Aspiration during the swallow – Incomplete closure of the vocal folds. Aspiration after the swallow – Incomplete elevation of the larynx results in the failure to clear all material from the pharynx. |
| Oesophageal | Describes the transport of the bolus through the oesophagus, consisting of muscle contractions to transport the bolus. | Loss of muscle contractions Stricture / obstruction |
If you would like further information, Rosemont provide a range of resources for healthcare professionals related to swallowing difficulties and the associated topic of medicine management, all available to view online. If you have any questions– please contact us.
ROS000051-003 DOP September 2025
- Dysphagia (difficulty swallowing). Available at: https://www.healthdirect.gov.au/dysphagia (Accessed September 2025)
- Guideline on the medication management of adults with swallowing difficulties. Available at: https://www.rosemontpharma.com/wp-content/uploads/2023/10/Wright-D-Chapman-N-Foundling-Miah-M-et-al.-Consensus-guideline-on-the-medication-management-of-adults-with-swallowing-difficulties.-Sept-2015.pdf (Accessed September 2025)
- Guideline on the medication management of adults with swallowing difficulties. Available at: https://www.rosemontpharma.com/wp-content/uploads/2023/10/Wright-D-Chapman-N-Foundling-Miah-M-et-al.-Consensus-guideline-on-the-medication-management-of-adults-with-swallowing-difficulties.-Sept-2015.pdf (Accessed September 2025)
- Wright et al. 2011. Prescribing Medicines for Patients with Dysphagia. A handbook for healthcare professionals.
- RCSLT Dysphagia – Guidance. Available at: https://www.rcslt.org/members/clinical-guidance/eating-drinking-and-swallowing/eating-drinking-and-swallowing-guidance/ (Accessed September 2025)